Health & Medicine
Your protective Igs: The major focus of COVID-19 vaccines


Antibody passports could be used to identify people who are vaccinated and are COVID-19 survivors. The body’s immune response helps guide which antibodies to look for in a ‘passport’

Published 4 September 2020
This article is the latest in a series of weekly columns about all things infection and immunity written by Nobel Laureate Professor Peter Doherty for the Doherty Institute, Setting It Straight.
Affinity we’ve met before when talking about the specific binding of Ig receptors to their complementary (cognate) antigens, but avidity, what’s that about?

Perhaps you recall the unique entertainment invented in New Zealand pubs where, after a glass or two, patrons wearing Velcro ‘sticky’ suits would run and jump to ‘attach’ as high as possible up a Velcro-covered wall.
Health & Medicine
Your protective Igs: The major focus of COVID-19 vaccines
Compare that spontaneous, slightly boozy, leap of faith to the elegant ascent of a stone-cold-sober, experienced mountaineer moving fast up a practice climbing wall.
As we all know from using, or misusing, Velcro fasteners, Velcro works by multiple, ‘low-affinity’ attachment points.
On the other hand, the placement of a skilled climber’s hands and feet represents a precise, limited, ‘high-affinity’ interaction. Both achieve the same end point, or ‘avidity of binding’, that allows a heavy human being to hang off a vertical wall!
The analogy in the immune response to SARS-CoV-2 is that the Velcro model represents the less-specific, ‘naïve’ IgM antibodies made first in any infection, while our climbers are the ‘educated’ IgGs and IgAs we’ve encountered previously.
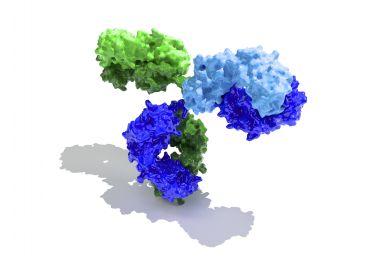
The IgMs are essentially five identical IgG ‘Y’ molecules (see Antibody dreaming essay). Think of five ‘synchronised swimmer’ quintuplets in a pool, with their feet together and their hands, the identical Ig variable (v) region binding sites, sticking out.

Compared with a ‘two-handed’, Y-shaped IgG ‘swimmer’, a single IgM quintuplet pentamer thus has the potential to interact with five-times as many antigens (spike proteins) on the surface of a SARS-CoV-2 virus particle.
Health & Medicine
Immunity to COVID-19: Lessons from malaria
As with our ‘Velcro jumpers’ and mountaineers, IgM attachment via a greater number of low-affinity, early response IgM V-regions can achieve an equivalent avidity of binding to that seen for the more mature, high-affinity IgG dimers.
With some viruses studied extensively in laboratory animals, an early IgM response can be protective, but we don’t yet know if that’s true for COVID-19. And in human influenza at least, virus-specific IgM is still being made, and detectable in blood, long after the virus is eliminated.
It’s also the case that engagement of five of the 10 IgM V-regions with, say, five of the 30+ spike proteins on the surface of a SARS-CoV-2 virus particle, can open out the IgM molecule in a way that activates the virus-destroying complement cascade. More of that later when we discuss the pathology of COVID-19.
All immune responses in previously unexposed people develop in the nurturing environment of lymph nodes, where the Ig V-regions on immunologically naïve B cells first encounter their cognate antigen, divide (clonal expansion), ‘class switch’ (from IgM to IgG) production and progressively change their functional status to make V-region ‘best fit’, high-affinity antibody molecules.
Any such response will continue in ‘active mode’ as long as there is antigen available and the B cells are receiving additional chemical signals from other lymphocytes called the CD4+ ‘helper’ T cells.

Health & Medicine
Lessons for a future pandemic
As all cells divide and replicate the ‘instructional’ DNA that it is passed down a clonal lineage, they run the risk of random nucleic acid changes, or mutations.
Exposure to the environmental, background radiation we all live with can promote the emergence of cancerous changes in any dividing cell type, while very high doses of ionizing radiation (such as those used in targeted cancer radiotherapy, or from a nuclear explosion) are, of course, lethal.
But the B cell is unique because it has a built-in, benign (in the sense of cell survival) molecular mechanism that drives what is called somatic hypermutation (SHM).
Operating only on the genes coding for the Ig V-region, SHM uses an enzyme called activation-induced cytidine deaminase to promote non-lethal changes in the replicating DNA.
As a consequence, we see the emergence of clonal ‘progeny’ in dividing, virus-specific B cell lineages that express mutant, ‘better-fit’ (for the target antigen), high-affinity Ig V-regions.

This process, which occurs only for B cells and not for T cells, is called ‘affinity maturation’. The consequence is the progressive selection of V-region-optimised IgG ‘sub-clones’ which go on to dominate and make a higher quality antibody response.
Health & Medicine
Modern lessons from our polio past
Being less specific, measuring IgM, either inadvertently or deliberately, can cause confusion when we do antibody surveys with less sensitive, rapid, blood pin-prick screening assays to measure the prevalence of prior SARS-CoV-2 infection in a community.
This is the reason for some of the confusion around background infection rates with COVID-19. Are we detecting ‘false positives’ due to cross-reactive, low-affinity IgM that could be a circulating ‘relic’ of prior exposure to, for example, one of the distantly related ‘common cold’ human coronaviruses?
That’s one reason why serological surveys in communities where there is minimal incidence of COVID-19 infection are hard to interpret: background cross-reactivity comes to the fore.
With regard to the idea of testing prior to the issue of ‘antibody passports’ to identify vaccines and COVID-19 survivors, IgM is not a problem providing we use one of the more sophisticated assays that tunes-out IgM to detect only virus-specific IgG.
At least from the purely technical aspect, antibody passports are feasible. But there are other complexities from the social and ethical aspects. And there are also doubts concerning the durability of the protective IgG response to COVID-19: we’ll get to some of that next week.
Banner: Getty Images