
Health & Medicine
Flattening the curve to help Australia’s hospitals prepare



Some countries have reported a 40 per cent decline in cancer cases at the peak of COVID-19, but an early GP visit means hospitals can prioritise care and capacity for cancer patients


Published 30 April 2020
We have witnessed massive changes in how we live since January 2020, with governments forcing strict regulations and urging people to socially isolate in an attempt to stop the unprecedented spread of COVID-19.
The immediate government response has focused on concerns about the limited capacity of the health service to manage the estimated increase in intensive care admissions.

While restrictions imposed by governments have been effective, a growing concern is what will happen in a post-COVID-19 era. One specific cause for concern is about falling rates of new cancer diagnoses.
The Netherlands Cancer Registry reported a decline in cancer incidence of up to 40 per cent per week on average in the last 14 weeks. In the UK, there has been a 75 per cent reduction in referrals for suspected cancer since the start of COVID-19 restrictions.
Health & Medicine
Flattening the curve to help Australia’s hospitals prepare
In Australia, cancer hospitals are also reporting reduced referrals of new patients. Although careful interpretation of this data is required, there is sufficient reason to flag this as an imminent policy problem.
Much of the work by government and many scientists involves the acute, emergency response to COVID-19 in order to ensure our health service capacity is sufficient to manage the increasing demand of people with severe infection.
However, with social distancing proving effective in controlling the immediate outbreak, another concern has arisen around the second and the third wave effects of the pandemic.
The second wave is known as the impact on urgent care for non-COVID-19 diseases and usually is explained by delays in access to health services.
The third wave reflects the impact of COVID-19 on care interruptions in chronic diseases and patients with known cancer. The latter is likely to occur because of changes in management of (metastatic) cancers receiving less (hospital based) chemotherapy.
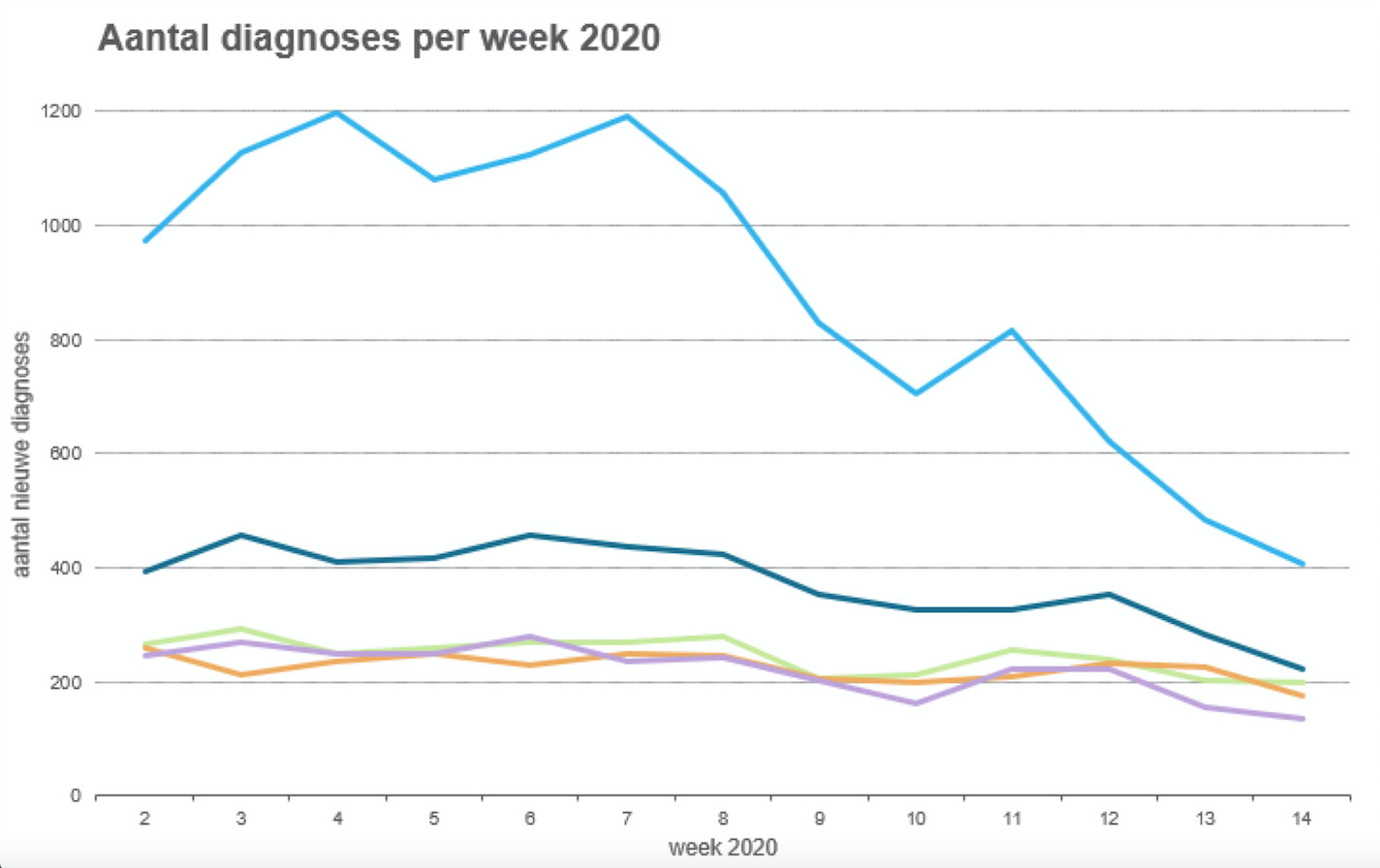
The Netherlands Cancer Registry routinely monitors cancer incidences during the pandemic and has reported declining cancer incidence rates up to 40 per cent at the peak of the COVID-19 outbreak, where the first case was reported on 27 February 2020.
According to the most recent data obtained on 29 April 2020, Dutch cancer incidences are returning to normal.
However, there are significant differences between cancer types, with breast cancer incidence remaining normal; but, skin cancers, male genitourinary cancers and blood cancer incidences still 30 to 40 per cent lower than normal.

Health & Medicine
Better cancer treatments from better data analysis
We should be aware that the Dutch data is not directly applicable to Australia as the https://www.rivm.nl/en/novel-coronavirus-covid-19/current-information-about-novel-coronavirus-covid-19as demonstrated by the COVID-19 infection and case-fatality rates.
Although there’s no specific Australian cancer incidence data during the emergence of the COVID-19 pandemic, there is related health service data which suggest Australia could experience similar declines.
Several reasons for a decline in cancer incidence can be identified, involving both patient and GP behaviours, which could explain the falling rates of cancer diagnosis.
The first is that patients may be more reluctant to attend general practice during the pandemic with symptoms possibly linked to cancer. There were early reports of reduced activity in general practice consistent with this theory.
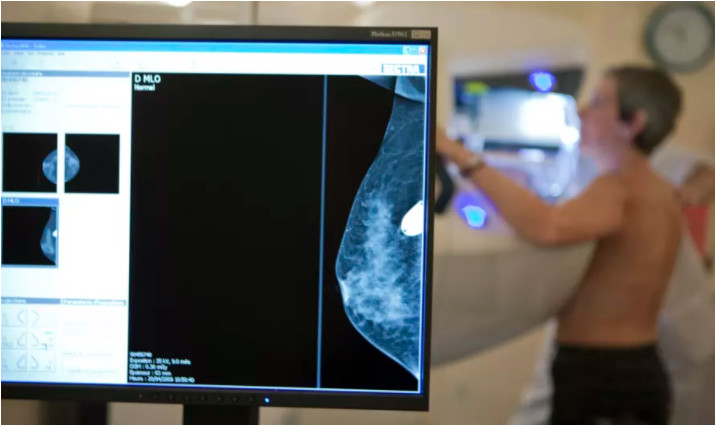
Lower participation in cancer screening will also reduce numbers of cancers detected, either because BreastScreen was suspended, or women not attending a cervical screening.
The switch to GP telehealth consultations could further impact the assessment of patients with cancer symptoms.
There have also been significant reductions in pathology and radiology tests. This could reflect the greater administrative challenges of ordering tests like these through telehealth, or that patients won’t leave home to have the tests performed.
GPs may also be more reluctant to refer patients for specialist diagnostic tests in an attempt to protect the health system.
Health & Medicine
The Global Cancer Atlas
A decline in cancer incidence is confirmed by hospitals reporting fewer referrals to specialised cancer care.
This could also explain why cancer incidence has dropped, as any diagnosis needs to be confirmed with pathological tests in labs which are already under pressure from COVID-19 testing.
But hospitals also report changes in routine clinical management of cancer patients, partly because patients fear being infected.
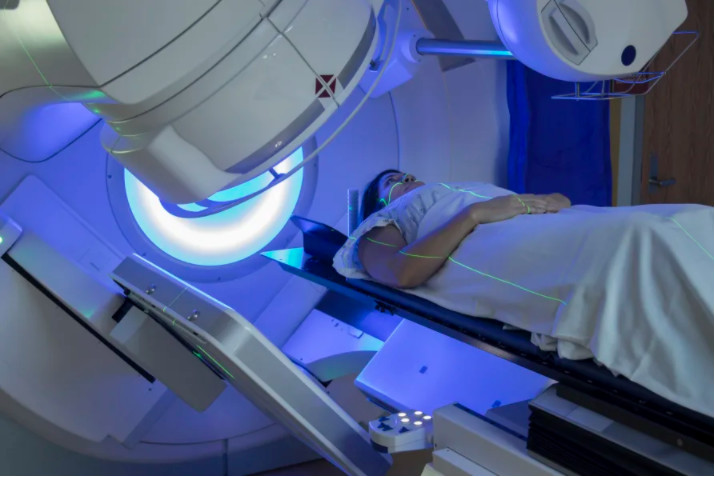
This has led to increase in teleconsultations, but also in delayed surgeries, utilising treatments that are less intense (such as fewer cycles of radiotherapy) or more home-based care (taking pills instead of intravenous chemotherapy) to reduce the risk of acquiring a hospital-based infection.
While hospitals are now planning to restore the delivery of care for cancer patients, it is likely that the capacity required for returning-to-normal routine care will be insufficient for some time to come.
For this reason, according to the European Society of Medical Oncology, priority should be particularly given to vulnerable patients with life-threatening disease, such as blood cancer patients, or patients in which an intervention is expected to result in overall survival gain.
Many professional societies are responding to the impact of COVID-19 on routine health services, and cancer specific guidelines have been issued by all large professional societies.
However, these have focused on the treatment of patients already diagnosed with cancer.

Health & Medicine
Improving cancer care through good communication
If Australia observes similar short-term falls in cancer incidence like the Dutch experience, we are likely to see a corresponding later surge in new cancer diagnoses as the COVID-19 restrictions are relaxed.
We expect that these delays in cancer incidence will significantly affect the survival of patients diagnosed during COVID times and have significant impacts on the health service capacity required to deal with later stage cancers.
Diagnostic delays are critical in determining the outcomes for many cancers. For instance, someone with a stage one lung cancer who experiences a diagnostic delay of about two months will be diagnosed with stage two lung cancer instead, with significant impact on overall survival.
But it also changes the demand for more extensive surgery, radiotherapy and systemic drug treatment.
It is insufficient to only talk about restarting elective treatments. Instead, we need to be analysing the potential impact of our response to COVID-19 on delays in cancer diagnosis, and prioritise the demand for cancer health services to maximise survival and quality of life.
Banner: Getty Images