Health & Medicine
Understanding epilepsy



Researchers are crowdsourcing mathematical whizzkids to help predict when a seizure might strike
Published 2 May 2017
When Dr Levin Kuhlmann (BSc(Hons) 2000) set about probing the mysteries of how and why epileptic seizures occur, he took a novel approach to advancing the cause.
He organised an international crowdsourcing project. He and his Melbourne colleagues sought engineering talent rather than investors’ money, with the goal of writing computer algorithms capable of predicting epileptic seizures based on the electrical signals and activity recorded from patients’ brains.
The project, with prize money of $US20,000, was sponsored by the University of Melbourne, the US National Institutes of Health, the American Epilepsy Society and MathWorks. It attracted 10,082 entries.
Melbourne is a world leader in the fight against the cruel and unpredictable disease of epilepsy. Much of that research owes its origins to the Bionics Institute and research there into the retrieval and interpretation of brain signals and the development of the cochlear implant – the bionic ear.
Members of that same team, centred in the University of Melbourne and the Royal Melbourne Hospital, went on to invent the bionic spine and then took up the challenge of epilepsy in collaboration with the University of Melbourne and St Vincent’s Hospital, Melbourne.
Dr Kuhlmann is a Research Fellow at the University’s Neuro-Engineering Laboratory in the Department of Electrical and Electronic Engineering.
For the competition we worked with data recorded at the University of Melbourne between 2010 and 2013 during a clinical trial of a brain implant device. We are trying to understand how seizures emerge in the brain while trying to develop algorithms that can predict seizures from changes in brain activity signals.
That’s assuming we can find a pattern or marker that is a reasonably reliable predictor of seizure. As we understand more about how seizures are generated we hope to improve the prediction of them and make the randomness more deterministic; more definable mathematically. The hope is to make seizures less like earthquakes, which can strike without warning, and more like hurricanes, where you have enough advance warning to seek safety. Basically, that’s the goal.
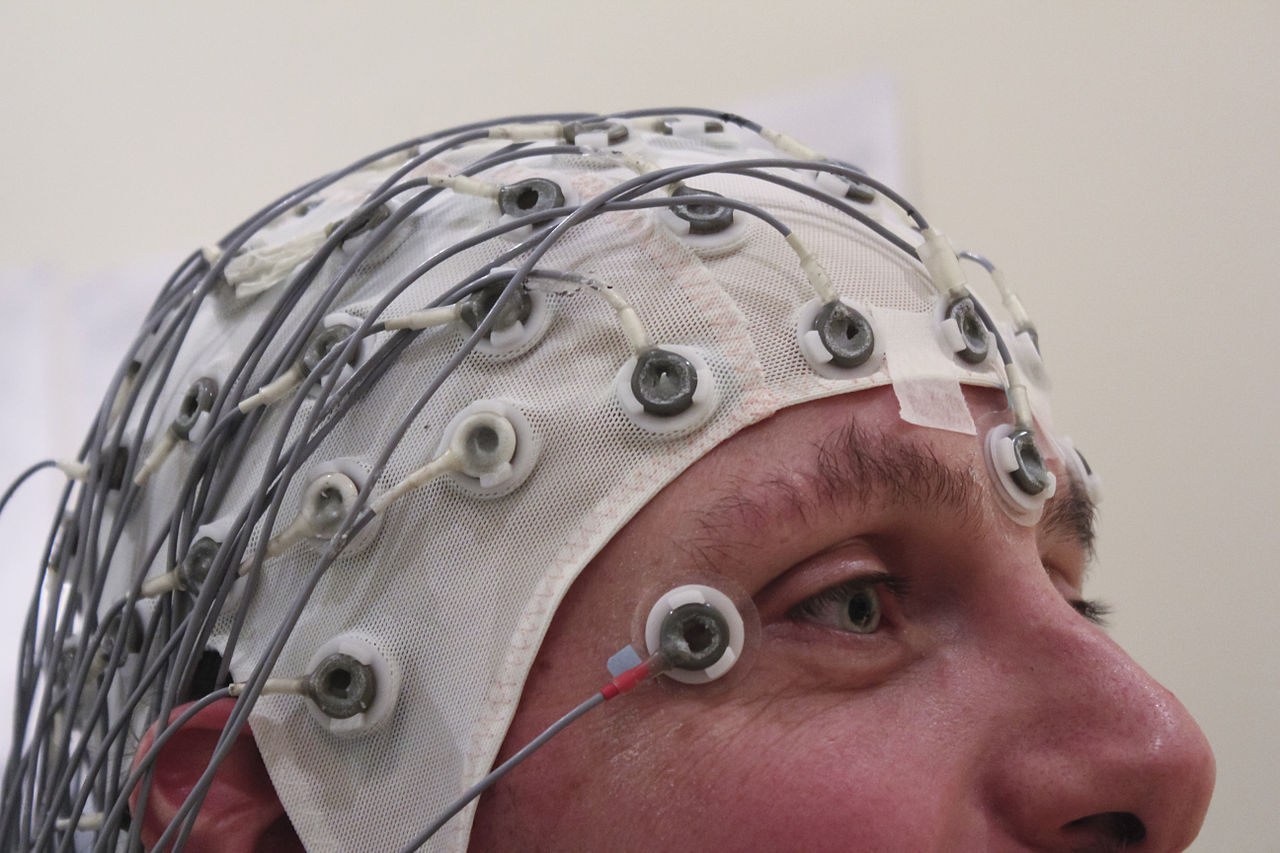
Yes. Epilepsy is highly different among individuals, very patient-specific. The types of epilepsy that people have can vary between groups and even within groups. Collection of data from patients, either by external sensors on the patient’s scalp, or by placing electrodes directly on the brain or deeply into it, has been done for some time, but accurate prediction of a seizure remains elusive.
Seizures seem to be random and come without warning, although a very few patients experience warning signs, called prodromes, of an imminent seizure. We think that to achieve successful prediction the algorithms will have to be trained for individual patients through machine-learning techniques, as has been done for years with speech-to-text, image recognition and other computer-based functions. Deep learning with neural networks is now a hot topic among researchers working on seizure prediction.
You need to collect data for a few months and then, with the patient, train the algorithm on that period of time. Once it is trained you let it run to see if it can predict seizures after that period.
The three prize-winning teams will publish their algorithms online on Kaggle for free access by anyone. Next, a post-contest assessment of the top 10 teams’ algorithms will be held, using data from at least 100 pre-seizure periods per patient. That’s important because it assesses the ability of the algorithms to work on large amounts of data they have not “seen” before. It helps us to ask, if we use the algorithms and train them on a patient for six months, will they continue to work years ahead?
Health & Medicine
Understanding epilepsy
If the post-contest assessment shows we can predict seizures on large amounts of “unseen” data for patients whose seizures have previously been difficult to predict, it will likely lead to new, larger long-term clinical trials of the algorithms and hopefully devices that can reliably give warnings of impending seizures or activate a brain implant that can control or avert seizures using electrical stimulation or drug delivery.
I am interested in how the brain works and finding a way to predict epileptic seizures is one of my areas of research. About 10 years ago, I worked at the Bionics Institute when researchers were beginning to think of branching out into other areas of medical bionics. In the meantime I went to Boston to do my PhD in computational modelling of vision and when I came back to the Institute the epilepsy project was underway.
Epilepsy is interesting because you get to study the whole brain dynamics and how the brain can change over time. It’s also a good way to study humans. Epilepsy is such a severe condition that people are willing to let you put electrodes in their brains to study it, although researchers also work with animals. Research has been done using dogs, which are vulnerable to epilepsy.
Research has been going on for about 20 years but around the late ’90s it started getting serious with a lot of international workshops held. The seventh of these was in Melbourne in 2015, a huge interdisciplinary effort with people from mathematics, physics, engineering, computer science, medicine, neurology and biology all trying to understand how and why seizures occur and the neurophysiology underlying it all.
More than 50 million people – about one per cent of the world’s population – are known to suffer from epilepsy, but some estimates put the figure as high as three per cent. Treatments currently range from medication to intracranial operations to remove parts of the brain affected by the disease. In both cases, side effects can produce problems such as loss of memory and physical and cognitive abilities. Also, about 30 per cent of patients are resistant to the current range of drugs. Seizures occur with abnormal, storm-like activity in the brain but vary widely.
Causes range from brain injuries to brain tumours and autism. Rwanda, for example, has one of the world’s highest rates of epilepsy, particularly among the thousands of child casualties of the war there. Brain damage to infants before or during birth can be a cause, as can strokes and infectious diseases such as AIDS, meningitis and viral encephalitis in older children and adults. It can even be genetic.
This story was first published in 3010 magazine.
Dr Kuhlmann acknowledges the expertise contributed to the project by Professor David Grayden (BE(Hons) 1990, BSc 1991, PhD 1999), deputy head of Electrical and Electronic Engineering and leader of the Bionics Laboratory at the Centre for Neural Engineering at the University, and by Professor Mark Cook (MB BS 1983), director of Neurology at St Vincent’s Hospital, Melbourne, an expert in epilepsy.
Banner image: Pixabay
